Clinical History
A seventy one year old male presents with atypical chest pain for past six months. He is unable to exercise due to severe knee arthritis and a dypridamole myocardial perfusion scan is arranged
by his LMO. (Figure One).
Scan Findings
Myocardial perfusion was imaged at rest and following a dypridamole infusion. These findings are typical of lateral wall ischaemia. The extent of this ischaemia is routinely quantified in terms of LV mass and expressed as a percentage of LV mass that is in jeopardy (Figure Two). As the extent of ischaemic myocardium was moderate at 7%, the patient was referred for coronary angiography with 90% stenosis in the circumflex artery being demonstrated.
Discussion
It used to be easy. If there was a significant stenosis in a coronary artery, the best treatment was a coronary angioplasty followed by insertion of a coronary stent. A recent study‐ the COURAGE study has suggested that medical therapy may be just as beneficial as the invasive treatment pathway. To say that the trial results are controversial is the understatement of the year. The COURAGE trial
took over 2000 patients with established coronary artery disease and randomised one group to optimal medical therapy and another group to optimal medical therapy plus angioplasty/stent. The
surprising result was that the patients randomised to the invasive pathway did not live longer than those treated just with medical therapy. A subgroup of COURAGE patients‐in both the invasive and non‐invasive pathways also had myocardial perfusion studies at the beginning of the study and 6‐18 months later. The extent of myocardial ischaemia at the time of diagnosis and the reduction in ischaemia with either therapy seem to be good predictors of prolonged survival.
Conclusion It is possible that not all patients with CAD need coronary artery stenting. Extensive myocardial ischaemia at the time of diagnosis or a failure to reduce this ischaemia with medical therapy may
provide a guideline to who needs invasive therapy.
Reference: Boden WE et al. Optimal medical therapy with or without PCI for stable coronary artery disease. N Engl J Med 2007; 356:1503‐16
Case Study submitted by
Patrick Butler
Department of Nuclear Medicine,
(PDF DOWNLOAD)
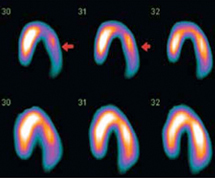
Figure 1.Selected horizontal axis images of left ventricular myocardial perfusion. The top row represents the stress images and the bottom row represents the rest images. Diminished perfusion in the lateral wall is seen in the stress images (arrows) with normal perfusion at rest.
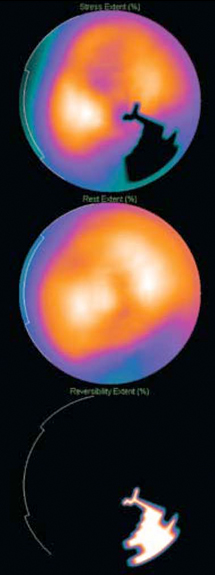
Figure 2. Software quantitative packages are
now available that permit an accurate calculation of the extent of myocardial ischaemia that is present. The first image is a computer map of the ischaemia at stress and
this is subtracted from the resting perfusion (image two) to give the extent of myocardial ischaemia (image three). There is a moderate ischaemic burden with 7%