This scan detects alterations in bone metabolism. Bone reacts to injury by taking calcium and phosphate from the circulation and depositing them at the site of the injury as a repair mechanism. This repair mechanism is much the same for most bone injuries such as fracture, infection, inflammation or tumour invasion. The radiotracer used in bone scans behaves like phosphate and mixes with the normal phosphate circulating in the bloodstream. Any time normal phosphate is deposited in the skeleton, so too is the tracer. There are several variations of bone scan that relate to the way the scan is performed:
1. Whole Body
In a whole body scan, the entire skeleton is imaged whereas in a regional scan, only the area of interest is imaged. The Nuclear Medicine Physician performing the scan usually looks at the whole body images and decides if additional images are needed for each patient.
Normal Whole Body Bone Scan
2. Three Phase
A particular part of the body is imaged while the tracer is being injected and also after a delay of two hours. The initial images relate to the blood flow in the region of the organ being imaged with the first set of images (phase one) showing arterial blood flow and the next set (phase two) showing venous flow also known as a ‘bloodpool image’. The delayed images (phase three) demonstrate uptake into the bone.
Three phase bone scan The first two rows of images are the first phase; the image at extreme right is the second phase; and the two bottom images are the third phase. There is marked hyperaemia to the posterior aspect of the right calcaneus (phases one and two) with increased bone uptake (phase three) at the same site. This is typical of a very active Achilles’ enthesopathy.
3. Tomography (SPECT).
This scan is analogous to a CT scan in that three dimensional data is acquired and then “sliced” in different imaging planes
to provide the best view. This type of imaging is also called SPECT which is an acronynm for Single Photon Emission Computed Tomography.
SPECT Images Coronal images of a lumbar bone scan. Each slice is one centimetre thick with the slices going from posterior to anterior. Transverse and saggital planes are also imaged with the same technique. The coronal plane is particularly useful in depicting facet joint pathology
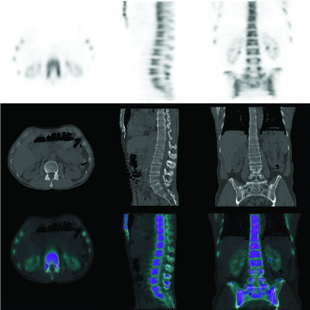
4. SPECT/CT A recent advance in Nuclear Medicine has been the development of an integrated machine that can take a nuclear medicine image almost simultaneously with a CT image. The enables the functional data from a nuclear medicine image to be superimposed on the anatomical data of a CT scan. This enhances the accuracy and reliability of the scan.
Normal Lumbar Spine SPECT/CT The top panel is a transverse slice, a saggital slice and a coronal slice of a bone scan of the lumbar spine. The middle panel is the corresponding CT though the same area. The bottom panel is a combination of the above scans with the bone scan in colour and the CT in black and white.
This all sounds very complicated for the referring doctor but the Nuclear Medicine Physician performing the scan performs the images that fit the clinical problem.
When do I order a bone scan?
1. Suspected Fracture when Radiographs Normal.
It is well established that normal radiographs miss fractures particularly at the following sites:
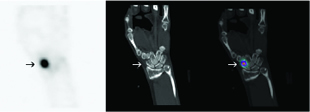
i) Scaphoid Fractures site of fracture. The middle image is the corresponding CT slice through same area. The right hand image is a combination of the above two with the bone scan in colour and the CT in black and white. This image confirms that the fracture on bone scan corresponds to the scaphoid.
ii) Talar Fracture
The left hand image is a sagittal slice of the bone scan through the middle of the talus with the arrow indicating the site of fracture. The middle image is the corresponding CT slice through the same area. The right hand image is a combination of the above two with the bone scan in colour and the CT in black and white. This image confirms that the fracture on the bone scan corresponds to the posterior talus.
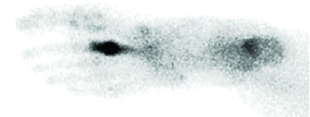
iii) Metatarsal Fractures
Plantar view of a bone scan showing marked focal accumulation of tracer in the mid shaft of the second left metatarsal with extension of tracer into the shaft of the metatarsal.
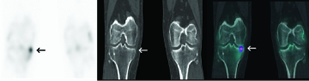
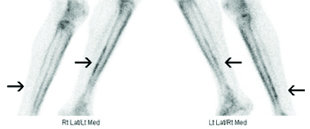
iv) Tibial Fracture
The left hand image is a coronal slice of the bone scan through the knees with the arrow indicating the site of fracture. The middle image is the corresponding CT slice through same area. The right hand image is a combination of the above two with the bone scan in colour and the CT in black and white. This image confirms that the fracture on bone scan corresponds medial tibial plateau.
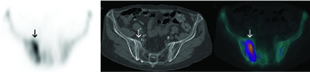
v) Sacral Fracture
The left hand image is a transverse slice of the bone scan through the sacrum with the arrow indicating the site of fracture. The middle image is the corresponding CT slice through same area. The right hand image is a combination of the above two with the bone scan in colour and the CT in black and white. This image confirms that the fracture on bone scan corresponds to the right sacral ala.
vi) Femoral Neck Fractures Pertrochanteric fracture of right proximal femur in a 90 year old woman who fell onto her right side 3 days ago. Radiographs showed osteoporosis of pelvis and femora with no Fracture.
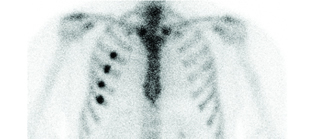
vii) Rib Fractures
Multiple rib fractures in 40 year old patient involved in motor vehicle accident. Persisting thoracic pain. Radiographs normal.
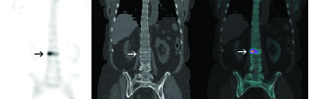
viii) Vertebral Fracture
The left hand image is a coronal slice of the bone scan through the lumbar spine with the arrow indicating the site of fracture. The middle image is the corresponding CT slice through same area. The right hand image is a combination of the above two with the bone scan in colour and the CT in black and white. This image confirms that the fracture on bone scan corresponds to the superior endplate of L2 vertebra.
2. Sports Injuries.
While bone scans are highly sensitive in detecting radiographically occult fractures, many soft tissue injuries can be detected:
i) Plantar Fasciitis
ii) Achilles’ Tendonitis
iii) Avulsion Injuries particularly in the foot and ankle
Ankle Fracture The left hand image is a coronal slice of the bone scan through the lower legs with the arrow indicating the site of fracture. The middle image is the corresponding CT slice through same area. The right hand image is a combination of the above two with the bone scan in colour and the CT in black and white. This image confirms that the fracture on bone scan corresponds to the lateral malleolus.
iv) Chronic strain injuries such as osteitis pubis
v) Shin splints and thigh splints vi) Apophysitis
3. Arthritis.
Bone scans are not routinely used in arthritis as most cases can be diagnosed and followed by clinical presentation alone. There are cases however where the bone scan can be of assistance. These instances include:
i) delineating the pattern and extent of changes to help identify the process involved e.g. predominantly peripheral small joints in rheumatoid arthritis versus large weight-bearing joints in osteoarthritis.
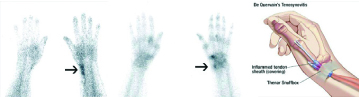
Tenosynovitis The left hand image is the initial flow images of a bone scan showing increased blood pool activity indicating inflammation in the radial aspect of the left wrist (arrow). The middle image shows faint increased uptake in the periosteal edge of the left distal radius in keeping with tenosynovitis. Low grade arthritis in the first CMC is also seen. The image on the right indicates the involved tendons in de Quervain’s tenosynovitis.
ii) in localising the particular joint inflamed for steroid injection.
iii) the sacro-iliac joints in ankylosing spondylitis and the temporo-mandibular joints as a cause for facial pain.
5. Metastatic Bone Disease.
Bone scanning is well established as the most sensitive technique for diagnosing metastatic bone disease and following progression. False negative bone scans occur in less than 2% of cases. Bone scans, however, are not always specific and X-ray examination of suspicious sites (scan directed) may be needed. X-rays are performed to see if there is an alternative, benign explanation for the bone scan abnormality. The presence of an abnormal scan with a normal X-ray
is highly suspicious
for metastasis.
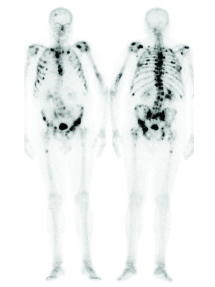
Widespread skeletal metastases in patient with prostate carcinoma.
6. Osteomyelitis. The bone scan has proven highly sensitive for osteomyelitis. The hallmark of acute osteomyelitis is focal arterial (early) hyperaemia combined with focally increased activity on blood pool and delayed scans. A gallium scan or white blood cell scan can be used to confirm the presence of infection and is particularly useful in complicated cases.
7. Paget’s Disease.
Bone scans define the extent of the disease.
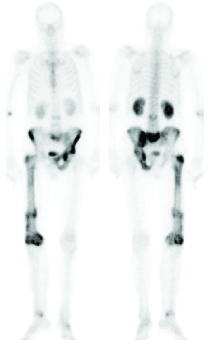
Paget’s disease in a 67 year old female who recently sustained a left femoral shaft fracture which required internal fixation.
8. Miscellaneous Skeletal Conditions.
The bone scan is also used in other clinical situations not often encountered in General Practice. These include primary bone tumours, avascular necrosis, reflex sympathetic dystrophy, the painful hip/knee prosthesis and metabolic bone disease.
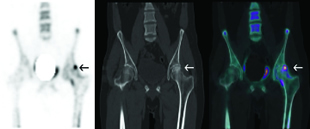
Avascular Necrosis of Femoral Head The left hand image is a coronal slice of the bone scan through the middle of the pelvis and femora with the arrow indicating a focal abnormality. The middle image is the corresponding CT slice through same area. The right hand image is a combination of the above two with the bone scan in colour and the CT in black and white. This image confirms that the focal abnormality on bone scan corresponds to the femoral head and is typical of avascular necrosis.
5. Metastatic Bone Disease.
Bone scanning is well established as the most sensitive technique for diagnosing metastatic bone disease and following progression. False negative bone scans occur in less than 2% of cases. Bone scans, however, are not always specific and X-ray examination of suspicious sites (scan directed) may be needed. X-rays are performed to see if there is an alternative, benign explanation for the bone scan abnormality. The presence of an abnormal scan with a normal X-ray
is highly suspicious
for metastasis.
Widespread skeletal metastases in patient with prostate carcinoma.
What do I tell the patient? Allow 3 hours.
No preparation required. In particular, the patient does not need to fast. Any recent radiograph should be brought to the Department.
The patient is given an intravenous injection of tracer and imaged 2 hours later. There are no restrictions on the patient during the two hour break.
What will the scan tell me?
The scan is a map of skeletal metabolism. Increased uptake indicates increased bone turnover and is the usual skeletal healing response to recent or active injury. The bone scan is read with a knowledge of the patient’s history as the accuracy of bone scan is significantly improved by careful imaging, an understanding of orthopaedics and an awareness of the clinical context.
What next?
If the bone scan is normal, then significant skeletal pathology such as fracture or metastatic disease is reasonably excluded and a new diagnosis must be sought. In patients with abnormal bone scans, often the diagnosis can be made with no further investigations, particularly in patients in whom radiographs were normal. On other occasions, further radiographs are needed to clarify the bone scan findings. This is particularly the case in patients with degenerative arthritis.