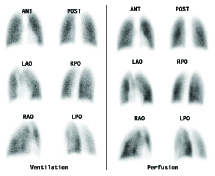
A lung scan, or V/Q scan, is performed to diagnose or exclude pulmonary embolism (PE).
The test is performed in two parts: 1. Ventilation (V) The patient breathes a radioactive aerosol or gas. Views of the lungs are then taken
in six projections.
2. Perfusion (Q) Technetium 99m-labelled macro aggregated albumin is injected into a peripheral vein.
These small aggregates then lodge in the small arterioles and give a good
representation of lung perfusion. Corresponding views to ventilation study are then performed.
Normal lung scan in a patient with pleuritic chest pain. A normal lung scan excludes pulmonary embolism.
Lung scan of patient with metastatic cancer presenting with syncope demonstrating massive pulmonary embolism.
When should I order a lung scan? PE is one of the hardest clinical diagnoses to make as there are no signs or symptoms that are specific for PE. Further, there are no laboratory, ECG or chest radiograph findings that can confidently confirm or exclude the diagnosis. Then there are the other tests such as Serum D-Dimer, V/Q scan, CTPA and leg ultrasounds and it can be confusing to know which test to order, in what sequence and when. In the main, pulmonary embolism is a “disease of the sick”, and most patients with PE have a predisposing condition to the development of PE. Unexplained chest pain and/or dyspnoea, particularly in a patient with one or more risk factors makes PE the diagnosis of exclusion.
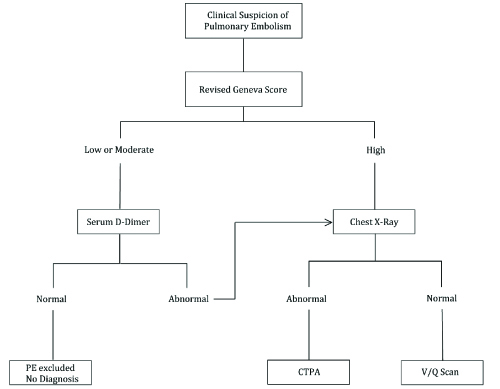
Flow chart for the investigation of a patient with a clinical suspicion of pulmonary embolism.
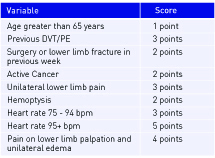
Step One: Assign a level of risk to the patient. done using a clinical prediction score. The best known of these is the Wells score or the Revised Geneva Score. In the Revised Geneva Score, a score is allocated for objective signs and symptoms that can be observed in the office.
The scoring is as on the left In those patients with a score of 0 to 3 points, PE is present in less than 10% of patients; in those with a score of 4 to 10 points, PE is present in about 30% of patients; and in those with a score of 11 or more, PE is present in about 75% of patients.
Step Two. Perform a serum D-Dimer test in those with low or moderate risk
If this is negative, then PE is excluded and a new diagnosis needs to be sought. In those patients with a high score and those with a low/moderate score but a positive serum D-Dimer, the next test is a Chest X-ray.
Step Three. Perform a CXR on the remaining patients
The patients in this group have a reasonable chance of having PE and must be investigated further and the next investigation is a Chest X-ray. In these patients with a normal CXR, V/Q scans are just as accurate as CTPA but have a much lower radiation dose to the patients. In patients with an abnormal CXR, CTPA is preferred even though the radiation dose is higher.
Step Four. Perform either a V/Q scan or a CTPA
A normal or low probability V/Q scan or a normal CTPA confidently excludes PE in most patients and an alternative diagnosis needs to be found. Similarly, a high probability V/Q scan or a positive CTPA confirms the diagnosis in most patients.
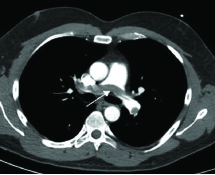
Positive CTPA Transverse slice through thorax demonstrating a saddle embolus in left and right pulmonary arteries (arrow).
What do I tell my patient?
Allow 1 hour.
No preparation required.
The patient takes 3-4 deep breaths of a specially prepared aerosol and then a series of images of the thorax will be taken. The patient then receives an intravenous injection and another series of images are taken. Usually a recently performed chest radiograph is also needed to fully interpret the scan.
What will the scan tell me?
The classical physiological change caused by a pulmonary embolus is decreased perfusion with normal ventilation—”V/Q mismatch”. Most pulmonary emboli are multiple and therefore a “high probability” scan result is one which demonstrates two or more areas (segments) of V/Q mismatch. In patients with a normal lung scan, the diagnosis of PE can be excluded with certainty and the search for a diagnosis should continue. It is known that patients with low probability scans have an excellent prognosis without anticoagulation and should not be treated. If there is a high clinical suspicion in a patient with a low probability scan, then a further testing should be performed. High probability scans confirm PE as the diagnosis and anticoagulation should be instituted in these patients.
What next?
Lung scanning is used to assess the results of therapy in patients diagnosed with PE. In patients with PE and with new or continuing symptoms, V/Q scanning is helpful in detected further emboli. A lung scan is often performed near the end of the period of anti-coagulation to assess the degree of resolution of the PE.
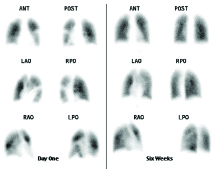
Right:
Six perfusion images on left demonstrate multiple perfusion defects. Ventilation scan (not shown) was normal with scan typical of multiple PE. Follow-up perfusion scan on right after anticoagulation therapy showing complete resolution of PE.