A 32 year old women presents to her local doctor complaining of twelve months history of recurrent abdominal pain. The pain typically occurs at night and is located in the right upper quadrant. The pain is of moderate to severe intensity and comes and goes over about an hour. The pain comes about once every 1-2 months. There is no associated vomiting or diarrhoea and the patient is well between attacks. Upper abdominal ultrasound is normal on two occasions with no evidence of gallstones. A hepatobiliary scan is ordered.
Scan Findings
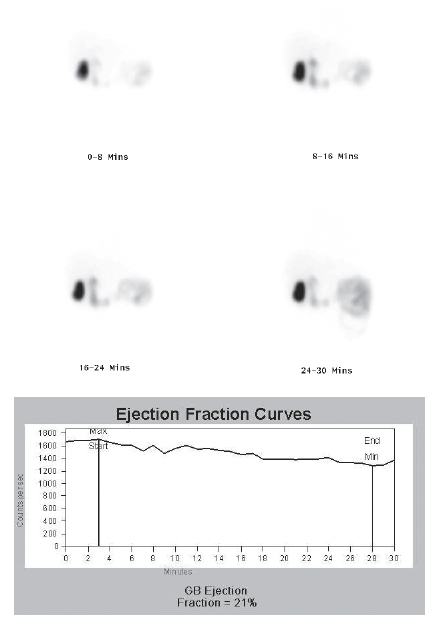
The scan shows that there is poor constriction of the gallbladder to CCK provocation. Normally, the gallbladder has an ejection fraction of greater than 35% in response to CCK.
Discussion
The clinical diagnosis of chronic cholecystitis is relatively straightforward with the patient complaining of symptoms of biliary colic with the ultrasound demonstrating gallstones with most patients being cured with cholecystectomy. It has been recognised that similar symptoms can be seen in patients without gallstones with the pain being caused by disturbed gallbladder physiology. The normal response to eating is for cholecystokinin (CCK) to be secreted from the stomach with the CCK resulting in dilatation of the Sphincter of Oddi and gallbladder constriction. It is thought that in these patients, there is a paradoxical response to CCK with the pain resulting from spasm of either the gallbladder, the Sphincter of Oddi or both structures. The hallmark of this entity is poor constriction of the gallbladder in response to CCK provocation with an abnormal gallbladder ejection fraction (GBEF)
Conclusion
In patients with typical symptoms of biliary colic with no gallstones, an abnormal gallbladder ejection fraction in response to CCK provocation is a good parameter of gallbladder dysfunction and strongly suggests that the patient will benefit from cholecystectomy.
Reference
Funch-Jensen, P. et al. Evaluation of the biliary tract in patient with functional biliary symptoms.
Word J Gastroenterol 2006; 12:2839-2845 Case Study submitted by
Patrick Butler
Department of Nuclear Medicine,
(PDF DOWNLOAD)
Figure 1: These are the images from the first part of the scan. The patient is injected with a radiolabelled bilirubin analogue with imaging performed over the upper abdomen. In normal fasting patients, there is uptake into the liver followed by excretion of tracer into the hepatic tracts, common bile duct, duodenum and gallbladder. By 60 minutes, maximal gallbladder filling is seen.
Figure 2. These are the images from the second part of the scan. At sixty minutes, an intravenous infusion of cholecystokinin (CCK) is administered with a further 30 minutes of imaging taking place. A Gallbladder Ejection fraction is then calculated . In normal patients, there is prompt gallbladder constriction with an ejectino fraction of at least 35%