Clinical History
A 33year old man presents with recurrent intermittent episodes of shortness of breath and palpitations. He is otherwise well. There is no past history of malignancy or venous thromboembolic disease, there has been no recent surgery or immobility, he has had no haemoptysis or calf symptoms and there is no history of cardiac or
respiratory disease. His cardio-respiratory examination is normal. An ECG and chest x-ray (Figure One) are normal, however a D-Dimer is elevated. A ventilation-perfusion lung scan is performed.
Scan Findings
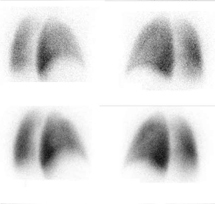
The lung scan is normal (Figure Two). There are no areas of ventilation - perfusion mismatch to indicate pulmonary embolism.
Discussion
A normal lung scan essentially rules out clinically
significant pulmonary embolism. In the clinical follow-up of patients with normal lung scans, pulmonary emboli almost never occur. In this patient, the clinical risk for pulmonary embolism was low. It is appropriate to measure the D-Dimer in low risk patients. This fibrinolytic breakdown product is elevated in venous thromboembolism and other conditions but when negative, virtually excludes pulmonary embolism in low risk patients. Surprisingly, the D-Dimer was elevated, which increased the patients clinical risk and therefore further testing was required to exclude pulmonary emboli. The optimal imaging test to perform for definitive diagnosis is in part dependent on the clinical history and chest x-ray findings. If there is a history of cardiopulmonary disease or the chest x-ray is abnormal, then CT pulmonary angiography is recommended. If the chest x-ray is normal and there is no history of cardiopulmonary disease, a lung scan can be performed, as the study in this scenario is likely to be diagnostic (high probability, low probability or normal) and less likely to be non-diagnostic (intermediate probability).
Conclusion
In the investigation of suspected pulmonary embolism, a normal lung scan effectively excludes this diagnosis. In the group of patients with no history of cardio-respiratory disease and with a normal chest x-ray, a lung scan is an acceptable next imaging test and is likely to be diagnostic, confirming or excluding pulmonary embolism. Case Study submitted by
Dr Scott Beuzeville
Department of Nuclear Medicine,
St. George Hospital.
(PDF DOWNLOAD)
Figure 1. Normal chest x-ray.
Figure 2.Lung scan demonstrating normal left and right posterior oblique images. There are no perfusion defects to suggest pulmonary emboli.