Clinical History
A previously well 55 year old male presents with the typical features of hyperthyroidism complaining of weight loss, marked lethargy and intermittent palpitations and tremor. The patient was clinically thyrotoxic with tachycardia, sweating palms and
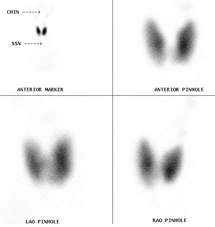
mild agitation. There was no neck tenderness, goiter or exophthalmos. Serum TSH was suppressed with elevated serum T4. A thyroid scan was performed (Figure One).
Scan Findings
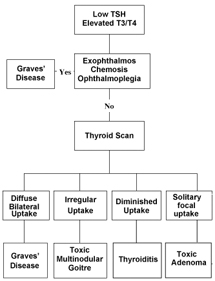
There are four main causes of thyrotoxicosis and these are sometimes difficult to differentiate clinically. It is important to make an accurate diagnosis of the cause of the thyrotoxicoisis as the prognosis and treatment is different for each underlying disease. A thyroid scan is a simple way to make the diagnosis as outlined in Figure Two.
Discussion
The classical description of Graves’ disease is so striking that the diagnosis can be made on clinical grounds alone. Unfortunately, the vast majority of patients with Graves’ disease do not present with the exophthalmos, periorbital swelling and inflammation and ophthalmoplegia. Contrary to popular teaching, patients with Graves’ disease often do not have a significantly enlarged thyroid gland. Once the diagnosis is made, patients are usually commenced on an anti-thyroid medication, in Australia this is usually neomercazole, and this
is maintained for at least 12 months in the hope of bringing the disease into a remission that may be life long. This is successful in about 50% of patients. In those who fail to go into remission or relapse following remission, further therapy with radioiodine therapy or surgery is needed.
Conclusion
In a thyrotoxic patient, a thyroid scan is usually needed to make the correct diagnosis of the underlying cause of the hyperthyroidism. Initial therapy for Graves’ Disease is an antithyroid medication with radioiodine administration or
surgery reserved for those patients who fail to respond or who relapse following therapy.
Reference:
Pearce EN. Diagnosis and management of thyrotoxicosis. BMJ 2006; 332:1369-1373.
Case Study submitted by
Dr Scott Beuzeville
Department of Nuclear Medicine,
St. George Hospital.
(PDF DOWNLOAD)
Figure 1. There is no preparation for a thyroid scan. A tracer that behaves like iodine is injected intravenously with imaging over the neck taking place 15-20 minutes later. In this patient, there is a diffuse increase in tracer uptake in both lobes of the thyroid gland in
keeping with Graves’ Disease.
Figure 2. Flow chart for the investigation of a patient with thyrotoxicosis.