This scan is also called a Sestamibi scan or a Thallium Scan. Myocardial perfusion scans estimate two cardiac aspects of cardiac physiology.
1. Myocardial Perfusion.
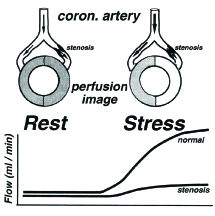
The scans measure the blood flow to the heart under both resting and stress conditions. Under normal conditions, the coronary arteries provide very little vascular resistance to blood flow with the principle site of vascular resistance being in the microcirculation. When a coronary artery becomes stenosed, resting blood flow is usually unaltered as the microcirculation dilates to overcome the stenosis. Resting myocardial blood flow remains normal until approximately 90% of the cross sectional area of the artery is occluded. So, even in severely stenosed coronary artery vessels, resting blood flow is usually maintained. The situation is different under stress conditions. Under stress conditions, either physical (i.e. exercise) or pharmacological (i.e. dipyridamole), blood flow through the stenosed vessel cannot increase and hence perfusion deteriorates and ischaemia
is produced.
When should I order this scan?
There are two groups of patients who benefit from Myocardial Perfusion Scans:
1. Does the patient have significant coronary artery disease? Generally, the first test used in this clinical scenario is an exercise ECG. Although this test has limited accuracy, it is inexpensive and widely available. However there are patients who cannot have the test and others whose diagnosis is not helped or even confused by the results of the exercise ECG. These patients are
a. Patients with who cannot exercise. These patients include those with painful joints, limited exercise tolerance and the aged who cannot manage on a treadmill. An exercise ECG is not helpful in excluding CAD if the patient cannot get to 85% of their predicted maximal heart rate.
b. Patients with equivocal exercise ECG
c. Patients with risk factors for CAD but normal exercise ECG
d. Patients with few factors for CAD with abnormal exercise ECG
e. Patients in whom interpretation of exercise ECG unreliable: • LV hypertrophy
• Left bundle branch block (LBBB)
• Digoxin effect
• Resting ST/T wave changes
• Females False positive exercise ECGs are seen far more commonly in young females and some authorities advocate a Myocardial Perfusion Scan as the initial investigation in females.
2. Does the patient with known Coronary Artery Disease have Ischaemia as a cause of this chest pain? In this clinical setting, exercise ECG is not sufficiently sensitive to exclude myocardial ischaemia and Myocardial Perfusion Scanning is used to detect the presence or absence of ischaemia and to provide an assessment of the significance of any
ischaemia found.
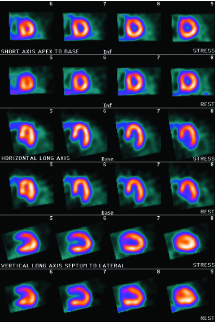
What will the scan tell me? There will be two sets of images depicting blood flow to the heart. The first set will demonstrate blood flow under stress conditions and the second blood flow under resting conditions. All imaging of the heart is now performed using tomographic techniques so that images like CT scans are produced. Tomographic imaging permits images of the heart in “slices” that are approximately 1 cm thick. These slices can be produced for any orientation but are usually done for three orientations: short axis slices; horizontal long axis slices; and vertical long axis slices.
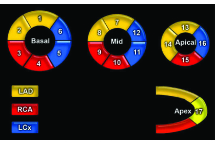
Myocardial Segments Representative drawings of short axis cardiac slices going from the apex of the heart on the left to the base on the right with a vertical long axis slice through the apex on the right. The vascular territories are shown on the bottom.
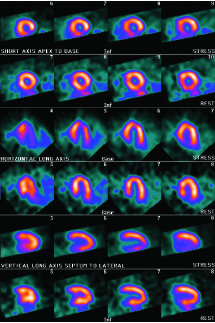
Representative images of a normal myocardial perfusion scan. There are three sets of paired images. The first two rows demonstrate stress and rest short axis slices; the middle two rows, stress and rest horizontal long axis slices and the last two rows, stress and rest vertical axis slices. The simplest way you view these images is to first inspect the top two rows ie. the stress and rest short axis slices. In these images, myocardial perfusion is relatively uniform so that the images should appear like a “doughnut”.
Myocardial perfusion scan on a 68 year old man with typical chest pain and a normal exercise ECG. On inspection of the stress and rest short axis slices, there is an inferior wall defect in the stress images that is not present in the rest images. This abnormality is confirmed by viewing the stress and rest vertical long axis slices. These appearances are typical of inferior wall ischaemia.
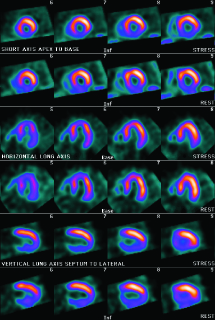
Myocardial perfusion scan on a 68 year old man with recent inferior myocardial infarction. On inspection of the stress and rest short axis slices, there is an inferior wall defect in the stress images that is also present in the rest images. This abnormality is confirmed by viewing the stress and rest vertical long axis slices. These appearances are typical of inferior wall infarction with no evidence of residual ischaemia post infarction.
What will I tell my patient?
This depends on whether the patient can exercise or not. If the patient can exercise, then he/she will have an exercise scan; if he/she is unable to exercise then the patient will have a dipyridamole myocardial scan.
1. Exercise.
Allow 3 hours.
The patient should fast from midnight before the scan. Also, if possible, beta-blockers, calcium channel antagonists and long acting nitrates should be withdrawn for at least 24-48 hours prior to the study so that the patient can be exercised optimally. Two sets of images are acquired. The patient is given an intravenous injection of tracer, and after about 30 minutes, the patient is imaged to obtain the rest myocardial perfusion images. The patient is then exercised on a treadmill just like a conventional exercise test (i.e. Bruce Protocol) and a second injection of tracer is given to the patient at peak exercise. The patient is then given a rest for about 30 minutes and the heart is then imaged to obtain the stress myocardial perfusion images.
2. Dipyridamole
Allow 3 hours.
The patient should fast from midnight before the scan and should refrain from drinking tea or coffee (caffeine) for 24 hours before the scan. Also, if possible, beta-blockers, calcium channel antagonists and long acting nitrates should be withdrawn for at least 24-48 hours prior to the study. As the effect of dipyridamole is reversed by aminophylline, patients should not be on methylxanthine products (e.g. theophylline) for at least 72 hours prior to the study. As with the exercise scan, a set of rest images are obtained first. The patient is then infused with dipyridamole, and tracer is injected about 3 minutes later which is corresponds to the time of peak dipyridamole effect. During the dipyridamole infusion, the patient may experience a “flushed” sensation. Imaging is performed as for the exercise stress scan.
How will the scan help me?
One of the commonest reasons that a patient visits a General Practitioner is for the investigation of chest pain. The primary concern of both the patient and the GP is whether this pain is cardiac or not. There are numerous tests that we can use to diagnose or exclude coronary artery disease. There are Exercise ECG’s, Myocardial Perfusion Scans, Stress Echocardiograms, CT Coronary Angiography and finally there is cardiac catherization. The problem for the General Practitioner is to work out which is the best test for which patient.
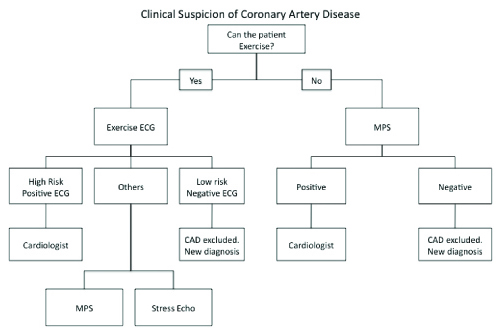
A simple flow chart is detailed below.
In the high risk patient with typical anginal chest pain, a positive Exercise ECG makes the diagnosis of CAD. In a low risk patient with atypical chest pain, a negative Stress ECG reasonably excludes CAD. In the main, these are the “simple” patients. Patients who don’t fall into this category are just as simple to evaluate. The next most appropriate test is either a Myocardial Perfusion Study or Stress Echocardiography. The accuracy of these tests are comparable although Stress Echocardiography is sometimes difficult to perform with overweight patients.
If this is positive, then the patient is 90% likely to have CAD and usually needs referral to a cardiologist; if negative, then the patient has less than 10% chance of CAD and another diagnosis needs to be found. In those patients who cannot exercise Myocardial Perfusion Scans with Dipyridamole are the best initial test to detect CAD and to define its significance.
What next?
This depends on whether the patient can exercise or not. If the patient can exercise, then he/she will have an exercise scan; if he/she is unable to exercise then the patient will have a dipyridamole myocardial scan.
1. Exercise.
In most patients, a positive scan usually results in referral to a cardiologist for an opinion as to whether the patient should undergo cardiac catherization or not. Conversely, a negative scan usually results in a search for an alternative diagnosis to CAD as a cause for that patient’s symptoms.
The Exercise Myocardial Perfusion Scan Guarantee.
Myocardial perfusion scans do not have a one hundred percent accuracy in the detection of CAD as compared to invasive coronary angiography. This aspect of myocardial perfusion scanning has been thoroughly investigated. Over 8,000 patients with a normal exercise myocardial perfusion scan were followed for three years. The annual cardiac event rate in these patients was 0.45% per year. Thus the patient with a normal exercise myocardial perfusion scan has a 98.8% chance of getting through the next three years without a cardiac event.
What about CT Coronary Angiography?
CTCA is a technique that is very promising in excluding CAD in low risk patients. It has not developed sufficiently to replace invasive coronary angiography and is relatively inaccurate in assessing the degree of stenosis in a diseased artery. While it is very popular in the United States as the initial test in excluding CAD in low risk patients, it’s clinical role is yet to be clearly defined in the Australian setting. It is significantly more expensive that exercise ECG and the radiation dose, particularly to young females is of some concern.